
Health Library
Malocclusion of teeth
Crowded teeth; Misaligned teeth; Crossbite; Overbite; Underbite; Open bite
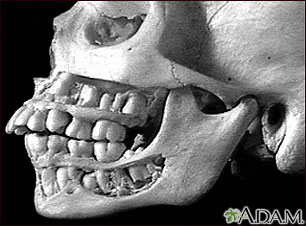
Malocclusion means the teeth are not aligned properly.
Images
I Would Like to Learn About:
Causes
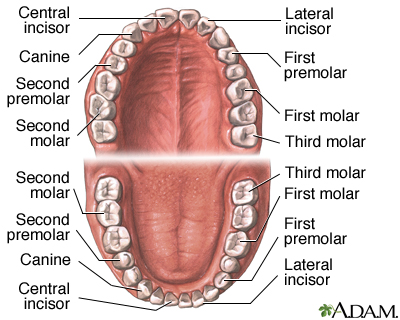
Occlusion refers to the alignment of teeth and the way that the upper and lower teeth fit together (bite). The upper teeth should fit slightly over the lower teeth. The points of the molars should fit the grooves of the opposite molar.
The upper teeth keep you from biting your cheeks and lips, and your lower teeth protect your tongue.
Malocclusion is most often hereditary. This means it is passed down through families. It may be caused by a difference between the size of the upper and lower jaws or between the jaw and tooth size. It causes tooth overcrowding or abnormal bite patterns. The shape of the jaws or birth defects such as cleft lip and palate may also be reasons for malocclusion.
Other causes include:
- Childhood habits such as thumb sucking, tongue thrusting, pacifier use beyond age 3, and prolonged use of a bottle
- Extra teeth, lost teeth, impacted teeth, or abnormally shaped teeth
- Ill-fitting dental fillings, crowns, dental appliances, retainers, or braces
- Misalignment of jaw fractures after a severe injury
- Tumors of the mouth and jaw
There are different categories of malocclusion:
- Class 1 malocclusion is the most common. The bite is normal, but the upper teeth slightly overlap the lower teeth.
- Class 2 malocclusion, called retrognathism or overbite, occurs when the upper jaw and teeth severely overlap the bottom jaw and teeth.
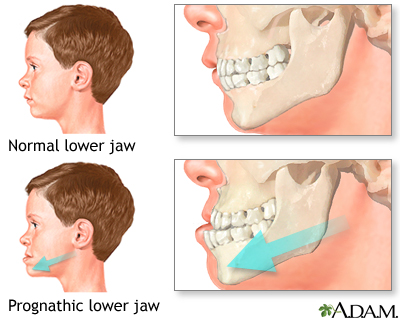
- Class 3 malocclusion, called prognathism or underbite, occurs when the lower jaw protrudes or juts forward, causing the lower jaw and teeth to overlap the upper jaw and teeth.
Symptoms
Symptoms of malocclusion are:
- Abnormal alignment of teeth
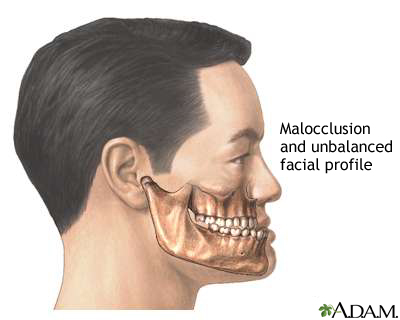
- Abnormal appearance of the face
- Difficulty or discomfort when biting or chewing
- Speech difficulties (rare), including lisp
- Mouth breathing (breathing through the mouth without closing the lips)
- Inability to bite into food correctly (open bite)
Exams and Tests
Most problems with teeth alignment are discovered by a dentist during a routine exam. Your dentist may pull your cheek outward and ask you to bite down to check how well your back teeth come together. If there is any problem, your dentist may refer you to an orthodontist for diagnosis and treatment.
You may need to have dental x-rays, head or skull x-rays, or facial x-rays. Diagnostic models of the teeth are often needed to diagnose the problem.
Treatment
Very few people have perfect teeth alignment. However, most problems are minor and do not require treatment.
Malocclusion is the most common reason for referral to an orthodontist.
The goal of treatment is to correct the positioning of the teeth. Correcting moderate or severe malocclusion can:
- Make teeth easier to clean and decrease risk of tooth decay and periodontal diseases (gingivitis or periodontitis).
- Eliminate strain on the teeth, jaws, and muscles. This lessens the risk of breaking a tooth and may reduce symptoms of temporomandibular joint disorders (TMJ).
Treatments may include:
- Braces or other appliances: Metal bands are placed around some teeth, or metal, ceramic, or plastic bonds are attached to the surface of the teeth. Wires or springs apply force to the teeth. Clear braces (aligners) without wires may be used in some people.
- Removal of one or more teeth: This may be needed if overcrowding is part of the problem.
- Repair of rough or irregular teeth: Teeth may be adjusted down, reshaped, and bonded or capped. Misshapen restorations and dental appliances should be repaired.
- Surgery: Surgical reshaping to lengthen or shorten the jaw is needed in rare cases. Wires, plates, or screws may be used to stabilize the jaw bone.
It is important to brush and floss your teeth every day and have regular visits to a general dentist. Plaque builds up on braces and may permanently mark teeth or cause tooth decay if it is not properly removed.
You will need a retainer to stabilize your teeth after having braces.
Outlook (Prognosis)
Problems with teeth alignment are easier, quicker, and less expensive to treat when they are corrected early. Treatment works best in children and adolescents because their bones are still soft and teeth are moved more easily. Treatment may last 6 months to 2 or more years. The time will depend on how much correction is needed.
Treatment of orthodontic disorders in adults is often successful, but may require longer use of braces or other devices.
Possible Complications
Complications of malocclusion include:
- Tooth decay
- Discomfort during treatment
- Irritation of mouth and gums (gingivitis) caused by appliances
- Chewing or speaking difficulty during treatment
When to Contact a Medical Professional
Call your dentist if toothache, mouth pain, or other new symptoms develop during orthodontic treatment.
Prevention
Many types of malocclusion are not preventable. It may be necessary to control habits such as thumb sucking or tongue thrusting (pushing your tongue forward between your upper and lower teeth). Finding and treating the problem early allows for quicker results and more success.
Related Information
Dental cavitiesGingivitis
Periodontitis
Cleft lip and palate
References
Dean JA, Walsh JS. Managing the developing occlusion. In: Dean JA, ed. McDonald and Avery's Dentistry for the Child and Adolescent. 11th ed. St Louis, MO: Elsevier; 2022:chap 23.
Dhar VK. Malocclusion. In: Kliegman RM, St. Geme JW, Blum, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 355.
Thumbigere-Math V, Hinrichs JE. The role of dental calculus and other local predisposing factors. In: Newman MG, Klokkevold PR, Elangovan S, Hemandez-Kapila YL, eds. Newman and Carranza's Clinical Periodontology and Implantology. 14th ed. Philadelphia, PA: Elsevier; 2023:chap 24.
Koroluk LD, Jackson TH. Adolescent patients. In: Stefanac SJ, Nesbit SP, eds. Diagnosis and Treatment Planning in Dentistry. 4th ed. St Louis, MO: Elsevier; 2024:chap 17.
Nesbit S, Reside J, Moretti A, et al. The definitive phase of treatment. In: Stefanac SJ, Nesbit SP, eds. Diagnosis and Treatment Planning in Dentistry. 4th ed. St Louis, MO: Elsevier; 2024:chap 11.
BACK TO TOPReview Date: 3/31/2024
Reviewed By: Michael Kapner, DDS, General Dentistry, Norwalk Medical Center, Norwalk CT. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
![]()