
Health Library
Metatarsus adductus
Metatarsus varus; Forefoot varus; In-toeing
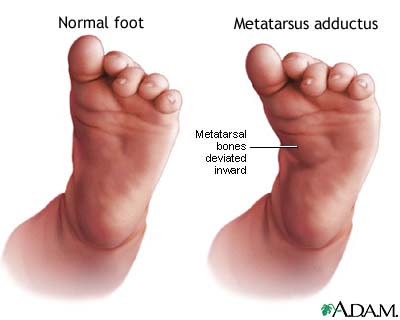
Metatarsus adductus is a foot deformity that occurs in infants. The bones in the front half of the foot bend or turn in toward the side of the big toe.
Images
I Would Like to Learn About:
Causes
Metatarsus adductus is thought to be caused by the infant's position inside the womb. Risks may include:
- The baby's bottom was pointed down in the womb (breech position).
- The mother had a condition called oligohydramnios, in which she did not produce enough amniotic fluid.
There may also be a family history of the condition.
Metatarsus adductus is a fairly common problem. It is one of the reasons why people develop "in-toeing."
Newborns with metatarsus adductus may also have a problem called developmental dysplasia of the hip (DDH), which allows the thigh bone to slip out of the hip socket.
Symptoms
The front of the foot is bent or angled in toward the middle of the foot. The back of the foot and the ankles are normal. About one half of children with metatarsus adductus have these changes in both feet.
(Club foot is a different problem. The foot is pointed down and the ankle is turned in.)
Exams and Tests
Metatarsus adductus can be diagnosed with a physical exam.
A careful exam of the hip should also be done to check for other causes of the problem.
Treatment
Treatment is rarely needed for metatarsus adductus. In most children, the problem corrects itself as they use their feet normally.
In cases where treatment is being considered, the decision will depend on how rigid the foot is when the health care provider tries to straighten it. If the foot is very flexible and easy to straighten or move in the other direction, no treatment may be needed. The child will be checked regularly. If the foot is very rigid, your provider may order other diagnostic tests.
In-toeing does not interfere with the child becoming an athlete later in life. In fact, many sprinters and athletes have in-toeing.
If the problem does not improve or your child's foot is not flexible enough, other treatments will be tried:
- Stretching exercises may be needed. These are done if the foot can be easily moved into a normal position. The family will be taught how to do these exercises at home.
- Your child may need to wear a splint or special shoes, called reverse-last shoes, for most of the day. These shoes hold the foot in the correct position.
Rarely, your child will need to have a cast on the foot and leg. Casts work best if they are put on before your child is 8 months old. The casts will probably be changed every 1 to 2 weeks.
Surgery is rarely needed. Most of the time, your provider will delay surgery until your child is between 4 and 6 years old.
A pediatric orthopedic physician should be involved in treating more severe deformities.
Outlook (Prognosis)
The outcome is almost always excellent. Almost all children will have a foot that works.
Possible Complications
A small number of infants with metatarsus adductus may have developmental dislocation of the hip. The hip condition should be monitored periodically.
When to Contact a Medical Professional
Contact your provider if you are concerned about the appearance or flexibility of your infant's feet.
Related Information
Developmental dysplasia of the hipReferences
Goodbody CM, Winell JJ, Davidson RS. The foot and toes. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 715.
Kelly DM. Congenital anomalies of the lower extremity. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 29.
McClincy MP, Olgun ZD, Dede O. Orthopedics. In: Zitelli BJ, McIntire SC, Nowalk AJ, Garrison J, eds. Zitelli and Davis' Atlas of Pediatric Physical Diagnosis. 7th ed. Philadelphia, PA: Elsevier; 2023:chap 22.
BACK TO TOPReview Date: 8/27/2024
Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
![]()