
Health Library
Hip joint replacement - series

Normal anatomy
The hip joint is made up of two major parts: the hip socket (a part of the pelvic bone called the acetabulum) and the beginning part of the thighbone (called the femur).

Indications
Osteoarthritis is the most common disease of the hip. It is caused by wear and tear on the joint. Cartilage is the firm, rubbery tissue that cushions your bones and joints. It allows bones to glide over one another. Cartilage can break down and wear away. As a result, the bones rub together, causing pain, swelling, and stiffness.
The most common reason to have a hip joint replaced is relieve severe arthritis pain that limits what you can do. Hip joint replacement is usually done in people age 60 and older. This is because most artificial hips do not last more than 20 years. Also, younger people who have this surgery tend to place more strain on their new hip.

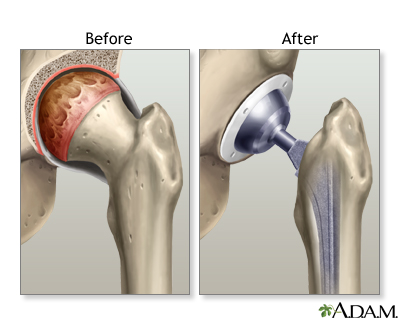
Procedure, part 1
Hip joint replacement is surgery to replace all or part of the hip joint with a man-made or artificial joint. The artificial joint is called a prosthesis. The artificial hip joint has 4 parts:
- A socket that replaces your old hip socket. The socket is usually made of metal.
- A liner that fits inside the socket. It is usually plastic, but some surgeons use ceramic and metal. The liner allows the hip to move smoothly.
- A metal or ceramic ball that will replace the round head (top) of your thighbone.
- A metal stem that is attached to the shaft of the bone.
After you receive anesthesia, your surgeon will make an incision (cut) to open up your hip joint. Then your surgeon will:
- Remove the head of your thigh (femur) bone.
- Clean out your hip socket and remove the remaining cartilage and damaged or arthritic bone.

Procedure, part 2
Next, the surgeon will:
- Put the new hip socket in place and insert the metal stem into your thighbone
- Check your hip's stability and place the correctly sized ball for the new joint
- Fix all the new parts in place, sometimes with a special cement
- Repair the muscles and tendons around the new joint
- Close the incision
A small drainage tube will be placed during surgery to help drain excess fluids from the joint area. A large dressing will cover to the hip area.
Aftercare
This surgery usually takes 1 to 3 hours. You will stay in the hospital for 3 to 5 days. Full recovery will take from 2 months to a year.
- Hip replacement surgery results are usually excellent. Most or all of the hip pain and stiffness should go away. Some people may have problems with infection, or even dislocation, of the new hip joint.
- Over time -- sometimes as long as 20 years -- the artificial hip joint will loosen. A second replacement may be needed.
- Younger, more active, people may wear out parts of their new hip. Their artificial hip may need to be replaced before it loosens. It is important to have scheduled follow-up visits with your surgeon every year to check the position of the implants.
By the time you go home, you should be able to walk with a walker or crutches without needing much help. Use your crutches or walker for as long as you need them. Most people do not need them after 2 to 4 weeks.
Keep moving and walking once you get home. Do not put weight on your side with the new hip until your doctor tells you it is okay. Start out with short periods of activity, and then gradually increase them. Your doctor or physical therapist will give you exercises to do at home.
Over time, you should be able to return to your former level of activity. You will need to avoid some sports, such as downhill skiing or contact sports like football and soccer. But you should be able to do low impact activities, such as hiking, gardening, swimming, playing tennis, and golfing.
Related Information
Hip joint replacementArthritis
Osteomalacia
BACK TO TOP
Review Date: 12/31/2023
Reviewed By: Neil J. Gonter, MD, Assistant Professor of Medicine, Columbia University, NY and private practice specializing in Rheumatology at Rheumatology Associates of North Jersey, Teaneck, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- 2024 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
![]()