
Health Library
Breast reconstruction - series
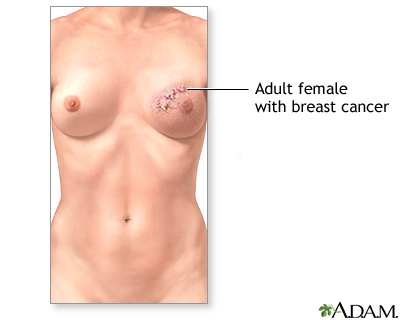
Indication, part 1
The normal female breasts are paired structures that contain fat and glandular tissue designed to secrete milk. Cancer of the breast is one of the more common cancers in women. Risk factors include a family history of breast cancer, early age at first period, and late menopause.
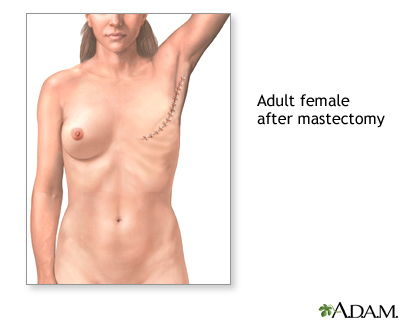
Indication, part 2
Breast removal (mastectomy), is performed most frequently for cancer of the breast. Occasionally, in patients with a strong family history of breast cancer and genetic abnormalities that predispose them to breast cancer, bilateral prophylactic mastectomies are performed to prevent the future occurrence of breast cancer.
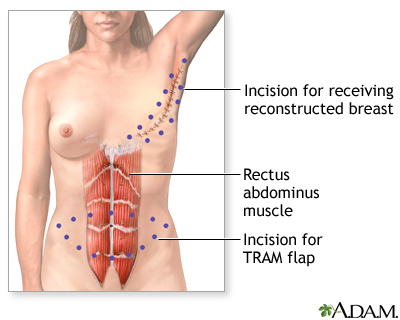
Incision
Reconstruction of the breast after mastectomy is performed in select patients who have very small tumors, or who undergo prophylactic (preventative) bilateral mastectomy. First, tissue from the lower abdomen, including skin, muscle, and blood vessels, is removed. This is called a TRAM flap.

Procedure, part 1
The flap is then transferred under the skin between the two sites, and sutured into place.

Procedure, part 2
Alternatively, a saline filled prosthesis can be implanted under the skin and muscle after mastectomy. Over the next few weeks and months, the prosthesis is slowly filled with increasing amounts of saline by injection, which expands the overlying skin and creates a breast mound.

Aftercare
The final step is nipple reconstruction. One method involves taking a partial graft from the remaining nipple to create a new one. In another method, the surgeon raises a small area of skin on the reconstructed breast and tattoos it at a later date. The overall results of breast reconstruction, while not perfect, are usually excellent. Nevertheless, patients should discuss their expectations with their surgeon at length prior to surgery.,
BACK TO TOP
Review Date: 3/11/2023
Reviewed By: Debra G. Wechter, MD, FACS, General Surgery Practice Specializing in Breast Cancer, Virginia Mason Medical Center, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- 2024 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
![]()