
Frozen shoulder
Adhesive capsulitis; Shoulder pain - frozen
Frozen shoulder is a condition in which the shoulder is painful and loses motion because of inflammation.
Causes
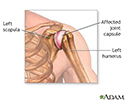
The capsule of the shoulder joint has ligaments that hold the shoulder bones to each other. When the capsule becomes inflamed, the shoulder bones are unable to move freely in the joint.
Most of the time, there is no cause for frozen shoulder. Women 40 to 70 years old are most affected, however, men can also get the condition.
Risk factors include:
- Diabetes
- Thyroid problems
- Changes in your hormones, such as during menopause
- Shoulder injury
- Shoulder surgery
- Open heart surgery
- Cervical disk disease of the neck


Symptoms
Main symptoms of a frozen shoulder are:
- Pain
- Decreased motion of the shoulder
- Stiffness
Frozen shoulder can start with pain without any cause or minor trauma. The pain may be severe and prevent you from moving your arm. This lack of movement can lead to stiffness and even less motion. Over time, you are not able to do movements such as reaching over your head or behind you.
Exams and Tests
Your health care provider will ask about your symptoms and examine your shoulder. A diagnosis is often made just with a clinical exam when you are not able to rotate your shoulder.
You may have x-rays of the shoulder. This is to make sure there is no other problem, such as arthritis or calcium deposits. Sometimes, an MRI exam shows inflammation, but these types of imaging tests are usually not needed to diagnose frozen shoulder.

Treatment
Pain is treated with NSAIDs and steroid injections. Steroid injections and physical therapy can improve your motion.
It can take a few weeks to see progress. It may take as long as 9 months to a year for complete recovery. Physical therapy may be intense and needs to be done every day.
Left untreated, the condition often gets better by itself within 2 years with little residual loss of motion. However, your other medical conditions may make the process last longer.
Risk factors for frozen shoulder, such as menopause, diabetes or thyroid problems, should also be treated.
Surgery is recommended if nonsurgical treatment is not effective. This procedure (shoulder arthroscopy) is done under anesthesia. During surgery the scar tissue is released (cut) by bringing the shoulder through a full range of motion. Arthroscopic surgery can also be used to cut the tight ligaments and remove the scar tissue from the shoulder. After surgery, you may receive pain blocks (shots) so you can do physical therapy.

Follow instructions on caring for your shoulder at home.
Outlook (Prognosis)
Treatment with physical therapy and NSAIDs often restores motion and function of the shoulder within a year. Even untreated, the shoulder may get better by itself in 2 years.
After surgery restores motion, you must continue physical therapy for several weeks or months. This is to prevent the frozen shoulder from returning. If you do not keep up with physical therapy, the frozen shoulder may come back.
Possible Complications
Complications may include:
- Stiffness and pain continue even with therapy
- The arm can break if the shoulder is moved forcefully during surgery
When to Contact a Medical Professional
If you have shoulder pain and stiffness and think you have a frozen shoulder, contact your provider for evaluation, referral, and treatment.
Prevention
Early treatment may help prevent stiffness. Call your provider if you develop shoulder pain that limits your range of motion for an extended period.
People who have diabetes or thyroid problems will be less likely to get frozen shoulder if they keep their condition under control.
References
American Academy of Orthopaedic Surgeons website. Frozen shoulder. orthoinfo.aaos.org/en/diseases--conditions/frozen-shoulder. Updated March 2018. Accessed January 12, 2023.
Barlow J, Mundy AC, Jones GL. Stiff shoulder. In: Miller MD, Thompson SR, eds. DeLee, Drez, & Miller's Orthopaedic Sports Medicine. 5th ed. Philadelphia, PA: Elsevier; 2020:chap 51.
Finnoff JT, Johnson W. Upper limb pain and dysfunction. In: Cifu DX, ed. Braddom's Physical Medicine and Rehabilitation. 6th ed. Philadelphia, PA: Elsevier; 2021:chap 35.
Miller RH, Azar FM, Throckmorton TW. Shoulder and elbow injuries. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 46.

Review Date: 12/12/2022
Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.