
Tricuspid atresia
Tri atresia; Valve disorder - tricuspid atresia; Congenital heart - tricuspid atresia; Cyanotic heart disease - tricuspid atresia
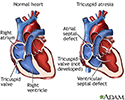
Tricuspid atresia is a type of heart disease that is present at birth (congenital heart disease), in which the tricuspid heart valve is missing or abnormally developed. The defect blocks blood flow from the right atrium to the right ventricle. Other heart or vessel defects are usually present at the same time.

Causes
Tricuspid atresia is an uncommon form of congenital heart disease. It affects about 5 in every 100,000 live births. One in five people with this condition will also have other heart problems.
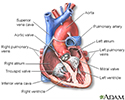
Normally, blood flows from the body into the right atrium, then through the tricuspid valve to the right ventricle and on to the lungs. If the tricuspid valve does not open, the blood cannot flow from the right atrium to the right ventricle. Because of the problem with the tricuspid valve, blood ultimately cannot enter the lungs. This is where it must go to pick up oxygen (becomes oxygenated).
Instead, the blood passes through a hole between the right and left atrium. In the left atrium, it mixes with oxygen-rich blood returning from the lungs. This mix of oxygen-rich and oxygen-poor blood is then pumped out into the body from the left ventricle. This causes the oxygen level in the blood to be lower than normal.
In people with tricuspid atresia, the lungs receive blood either through a hole between the right and left atria (described above), or through maintenance of a fetal vessel called the ductus arteriosus. The ductus arteriosus connects the pulmonary artery (artery to the lungs) to the aorta (main artery to the body). It is present when a baby is born, but normally closes by itself shortly after birth.
Symptoms
Symptoms include:
- Bluish color to the skin (cyanosis) due to low oxygen level in the blood
- Fast breathing
- Fatigue
- Poor growth
- Shortness of breath

Exams and Tests
This condition may be discovered during routine prenatal ultrasound imaging or when the baby is examined after birth. Bluish skin is present at birth. A heart murmur is often present at birth and may increase in loudness over several months.

Tests may include the following:
- ECG
- Echocardiogram
- Chest x-ray
- Cardiac catheterization
- MRI of the heart
- CT scan of the heart




Treatment
Once the diagnosis is made, the baby will often be admitted to the neonatal intensive care unit (NICU). A medicine called prostaglandin E1 may be used to keep the ductus arteriosis open (patent) so that blood can circulate to the lungs.
Generally, patients with this condition require surgery. If the heart is unable to pump enough blood out to the lungs and rest of the body, the first surgery most often takes place within the first few days of life. In this procedure, an artificial shunt is inserted to keep blood flowing to the lungs. In some cases, this first surgery is not needed.
Afterward, the baby goes home in most cases. The child will need to take one or more daily medicines and be closely followed by a pediatric cardiologist. This doctor will decide when the second stage of surgery should be done.
The next stage of surgery is called the Glenn shunt or hemi-Fontan procedure. This procedure connects half of the veins carrying oxygen-poor blood from the upper half of the body directly to the pulmonary artery. The surgery is most often done when the child is between 4 to 6 months old.
During stage I and II, the child may still look blue (cyanotic).
Stage III, the final step, is called the Fontan procedure. The rest of the veins carrying oxygen-poor blood from the body are connected directly to the pulmonary artery leading to the lungs. The left ventricle now only has to pump to the body, not the lungs. This surgery is usually performed when the child is 18 months to 3 years old. After this final step, the baby's skin is no longer blue.
Outlook (Prognosis)
In most cases, surgery will improve the condition.
Possible Complications
Complications may include:
- Irregular, fast heart rhythms (arrhythmias)
- Chronic diarrhea (from a disease called protein-losing enteropathy)
- Heart failure
- Fluid in the abdomen (ascites) and in the lungs (pleural effusion)
- Blockage of the artificial shunt
- Strokes and other nervous system complications
- Sudden death
When to Contact a Medical Professional
Contact your health care provider right away if your infant has:
- New changes in breathing patterns
- Problems eating
- Skin that is turning blue
Prevention
There is no known way to prevent tricuspid atresia.
Women who plan to become pregnant should be immunized against rubella if they are not already immune. Rubella infection in a pregnant woman can cause congenital heart disease.
Women who are pregnant should get good prenatal care:
- Avoid alcohol and illegal drugs during pregnancy.
- Tell your provider that you are pregnant before taking any new medicines.
- Have a blood test early in your pregnancy to see if you are immune to rubella. If you are not immune, avoid any possible exposure to rubella and get vaccinated right after delivery.
- Pregnant women who have diabetes should try to get good control over their blood sugar level.
Some inherited factors may play a role in congenital heart disease. Many family members may be affected. If you are planning to get pregnant, talk to your provider about screening for genetic diseases.
References
Valente AM, Dorfman AL, Babu-Narayan SV, Kreiger EV. Congenital heart disease in the adolescent and adult. In: Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia, PA: Elsevier; 2022:chap 82.
Well A, Fraser CD. Congenital heart disease. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. St Louis, MO: Elsevier; 2022:chap 59.
Heart - section through the middle - illustration
Heart - section through the middle
illustration
Tricuspid atresia - illustration
Tricuspid atresia
illustration
Review Date: 10/23/2023
Reviewed By: Michael A. Chen, MD, PhD, Associate Professor of Medicine, Division of Cardiology, Harborview Medical Center, University of Washington Medical School, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.