
Bowel incontinence
Uncontrollable passage of feces; Loss of bowel control; Fecal incontinence; Incontinence - bowel
Bowel incontinence is the loss of bowel control, causing you to unexpectedly pass stool. This can range from sometimes leaking a small amount of stool and passing gas, to not being able to control bowel movements.
Urinary incontinence is when you are not able to control passing urine. It is not covered in this article.

Considerations
In adults age 65 and older, women tend to have problems with bowel control more often than men.
Children who have problems with leakage due to toilet training problems or constipation may have encopresis.
The rectum, anus, pelvic muscles, and nervous system must work together to control bowel movements. If there is a problem with any of these, it can cause incontinence. You must also be able to recognize and respond to the urge to have a bowel movement.
Many people feel embarrassed about bowel incontinence and may not tell their health care provider. But incontinence can be treated. So you should tell your provider if you are having problems. Proper treatment can help most people gain control of their bowels. Exercises to make the anal and pelvic muscles stronger can help the bowels work properly.
Causes
Reasons people have bowel incontinence include:
- Ongoing (chronic) constipation. This causes the anal muscles and intestines to stretch and weaken, leading to diarrhea and stool leakage.
- Fecal impaction. It is most often caused by chronic constipation. This leads to a lump of stool that partly blocks the large intestine.
- Long-term laxative use.
- Colectomy or bowel surgery.
- Not sensing that it's time to have a bowel movement.
- Emotional problems.
- Gynecological, prostate, or rectal surgery.
- Injury to the anal muscles due to childbirth (in women).
- Nerve or muscle damage (from injury, tumor, or radiation).
- Severe diarrhea that causes leakage.
- Severe hemorrhoids or rectal prolapse.
- Stress of being in an unfamiliar environment.

Home Care
Often, simple changes may help reduce bowel incontinence. Your provider may suggest one or more of these treatments.
Diet -- Track the foods you eat to see if any types of foods cause problems. Foods that may lead to incontinence in some people include:
- Alcohol
- Caffeine
- Dairy products (in people who are unable to digest lactose, a sugar found in most dairy products)
- Fatty, fried, or greasy foods
- Spicy foods
- Cured or smoked meats
- Sweeteners such as fructose, mannitol, sorbitol, and xylitol

Fiber -- Adding bulk to your diet may thicken loose stool. To increase fiber:

- Eat more whole grains. Aim for 30 grams of fiber a day. Read food labels to see how much fiber is in breads, cereals, and other foods.
- Use products such as Metamucil that have a type of fiber called psyllium, which adds bulk to stools.
Bowel retraining and pelvic floor exercises -- These methods can help you control your anal sphincter muscle when you have a bowel movement. Your provider can show you exercises to strengthen the pelvic floor and anal muscles. Bowel retraining involves trying to have a bowel movement at certain times of the day.
Some people can't tell when it's time to have a bowel movement. Sometimes they can't move well enough to safely get to the toilet on their own. These people need special care. They may become used to not getting to the toilet when it's time to have a bowel movement. To prevent this problem, help them get to the toilet after meals and when they feel the urge. Also, make sure the bathroom is safe and comfortable.

Using special pads or undergarments can help an incontinent person feel safe when they leave home. You can find these products in pharmacies and in many other stores.
SURGERY
If treatment does not work, surgery may help correct the problem. There are several types of procedures. The choice of surgery is based on the cause of the incontinence and the person's general health.
Anal sphincter repair -- This surgery may help people whose anal muscle ring (sphincter) isn't working well due to injury or aging. The anal muscles are reattached to tighten the sphincter and help the anus close more completely.
Gracilis muscle transplant -- In people who have lost nerve function in the anal sphincter, gracilis muscle transplants may help. The gracilis muscle is taken from the inner thigh. It is put around the sphincter to help tighten the sphincter muscle.
Artificial bowel sphincter -- The artificial sphincter consists of 3 parts: a cuff that fits around the anus, a pressure-regulating balloon, and a pump that inflates the cuff.
During surgery, the artificial sphincter is placed around the anal sphincter. The cuff stays inflated to maintain continence. You have a bowel movement by deflating the cuff. The cuff will automatically re-inflate in 10 minutes.
Sacral nerve stimulator -- A device can be put inside the body to stimulate the nerves that maintain continence.
Fecal diversion -- Sometimes, this procedure is performed in people who are not helped by other therapies. The large intestine is attached to an opening in the abdominal wall called a colostomy. Stool passes through this opening to a special bag. You will need to use a colostomy bag to collect stool most of the time.
Injection treatment -- This procedure injects a thick gel (Solesta) into the anal sphincter to bulk it up.
If treatment does not get rid of bowel incontinence, you can use special fecal collection devices to contain the stool and protect your skin from breakdown. These devices have a drainable pouch attached to an adhesive wafer. The wafer has a hole cut through the center, which fits over the opening to the anus.
When to Contact a Medical Professional
Report any problems with incontinence to your provider. Contact your provider if:
- A child who has been toilet trained has any stool incontinence
- An adult has stool incontinence
- You have skin irritation or sores as a result of bowel incontinence
- You have severe diarrhea
What to Expect at Your Office Visit
Your provider will take your medical history. Be sure to tell your provider about all the prescription and over-the-counter medicines you take. Taking antacids or laxatives can cause bowel incontinence, particularly in older people.
Your provider will also perform a physical exam, focusing on your stomach area and rectum. Your provider will insert a lubricated finger into your rectum to check sphincter tone and anal reflexes, and to look for any problems.
Diagnostic tests may include:
- Barium enema
- Blood tests
- Colonoscopy
- Electromyography (EMG)
- Rectal or pelvic ultrasound
- Stool culture
- Test of anal sphincter tone (anal manometry)
- X-ray procedure using a special dye to evaluate how well the sphincter contracts (balloon sphincterogram)
- X-ray procedure using a special dye to see the bowel while you have a bowel movement (defecography)




References
Madoff RD, Melton-Meaux GB. Diseases of the rectum and anus. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier; 2020:chap 136.
Rao SSC. Fecal incontinence. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 18.
Digestive system - illustration
Digestive system
illustration
Inflatable artificial sphincter - illustration
Inflatable artificial sphincter
illustration
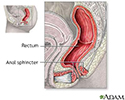
Anal sphincter anatomy - illustration
Anal sphincter anatomy
illustration


Review Date: 10/31/2022
Reviewed By: Michael M. Phillips, MD, Emeritus Professor of Medicine, The George Washington University School of Medicine, Washington, DC. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.