
Rotator cuff repair
Surgery - rotator cuff; Surgery - shoulder - rotator cuff; Rotator cuff repair - open; Rotator cuff repair - mini-open; Rotator cuff repair - laparoscopic
Rotator cuff repair is surgery to repair a torn tendon in the shoulder. The procedure can be done with a large (open) incision or with shoulder arthroscopy, which uses smaller incisions.

Description

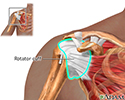
The rotator cuff is a group of muscles and tendons that form a cuff over the shoulder joint. These muscles and tendons hold the arm in its joint and help the shoulder joint to move in a coordinated and pain free way. The tendons can be torn from overuse, injury, or wearing away over time.
You will likely receive general anesthesia before this surgery. This means you will be asleep and unable to feel pain. Or, you will have regional anesthesia. Your arm and shoulder area will be numbed so that you do not feel any pain. If you receive regional anesthesia, you will also be given medicine to make you very sleepy during the operation.
Three common techniques are used to repair a rotator cuff tear:
- During open repair, a surgical incision is made and a large muscle (the deltoid) is gently moved out of the way to do the surgery. Open repair is done for large or more complex tears.
- During arthroscopy, the arthroscope is inserted through a small incision. The scope is connected to a video monitor. This allows the surgeon to view the inside of the shoulder. One to three additional small incisions are made to allow other instruments to be inserted.
- During mini-open repair, any damaged tissue or bone spurs are removed or repaired using an arthroscope. Then during the open part of the surgery, a 2- to 3-inch (5 to 7.5 centimeters) incision is made to repair the rotator cuff.
To repair the rotator cuff:
- The tendons are re-attached to the bone.
- Small rivets (called suture anchors) are often used to help attach the tendon to the bone. The suture anchors can be made of metal or material that dissolves over time, and do not need to be removed.
- Sutures (stitches) are attached to the anchors, which tie the tendon back to the bone.
At the end of the surgery, the incisions are closed, and a dressing is applied. If arthroscopy was performed, most surgeons take pictures of the procedure from the video monitor to show you what they found and the repairs that were made.
Why the Procedure Is Performed
Reasons rotator cuff repair may be done include:
- You have shoulder pain when you rest or at night, and it has not improved with a specific exercise program (physical therapy) over 3 to 4 months.
- You are active and use your shoulder for sports or work.
- You have weakness and are unable to do everyday activities.
Surgery is a good choice when:
- You have a complete rotator cuff tear.
- A tear was caused by a recent injury.
- Several months of physical therapy hasn't improved your symptoms.
- The tear is causing significant loss of function and symptoms.
A partial tear may not require surgery. Instead, rest and exercise are used to heal the shoulder. This approach is often best for people who do not place a lot of demand on their shoulder. Pain can be expected to improve. However, the tear can become larger over time.
Risks
Risks of anesthesia and surgery in general are:
- Allergic reactions to medicines
- Problems breathing
- Bleeding, blood clots, infection
Risks of rotator cuff surgery are:
- Failure of surgery to relieve symptoms
- Injury to a tendon, blood vessel, or nerve
Before the Procedure
Tell your health care provider what medicines you are taking. This includes medicines, supplements, or herbs you bought without a prescription.
During the 2 weeks before your surgery:
- You may be asked to temporarily stop taking blood thinners. These include aspirin, ibuprofen (Advil, Motrin), naproxen (Naprosyn, Aleve), and other medicines.
- Ask your surgeon which medicines you should still take on the day of your surgery.
- If you have diabetes, heart disease, or other medical conditions, your surgeon will ask you to see your provider who treats you for these conditions.
- Tell your provider if you have been drinking a lot of alcohol, more than 1 or 2 drinks a day.
- If you smoke, try to stop. Ask your provider for help. Smoking can slow wound and bone healing.
- Tell your surgeon if you develop a cold, flu, fever, herpes breakout, or other illness before your surgery. The procedure may need to be postponed.
On the day of surgery:
- Follow instructions on when to stop eating and drinking before the surgery.
- Take the medicines your surgeon told you to take with a small sip of water.
- Follow instructions on when to arrive at the hospital. Be sure to arrive on time.
After the Procedure
Follow any discharge and self-care instructions you are given.
You will be wearing a sling when you leave the hospital. Some people also wear a shoulder immobilizer. This keeps your shoulder from moving. How long you wear the sling or immobilizer will depend on the type of surgery you had.
Recovery can take 4 to 6 months, depending on the size of the tear and other factors. You may have to wear a sling for 4 to 6 weeks after surgery. Pain is usually managed with medicines.
Physical therapy can help you regain the motion and strength of your shoulder. The length of therapy will depend on the repair that was done. Follow instructions for any shoulder exercises you are told to do.

Outlook (Prognosis)
Surgery to repair a torn rotator cuff is often successful in relieving pain in the shoulder. The procedure may not always return strength to the shoulder. Rotator cuff repair can require a long recovery period, especially if the tear was large.
When you can return to work or play sports depends on the surgery that was done. Expect several months to resume your regular activities.
Some rotator cuff tears may not fully heal. Stiffness, weakness, and chronic pain may still be present.
Poorer results are more likely when the following are present:
- The rotator cuff was already torn or weak before the injury.
- The rotator cuff muscles have severely weakened before surgery.
- Larger tears.
- After-surgery exercise and instructions are not followed.
- You're over age 65.
- You smoke.
References
Klein JS, Leggin BG, Namdari S, Williams GR. Rotator cuff tendinopathies and tears: surgery and therapy. In: Skirven TM, Osterman AL, Fedroczyk JM, Amadio PC, Feldscher SB, Shin EK, eds. Rehabilitation of the Hand and Upper Extremity. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 38.
Mosich GM, Yamaguchi KT, Petrigliano FA. Rotator cuff and impingement lesions. In: Miller MD, Thompson SR, eds. DeLee, Drez & Miller's Orthopaedic Sports Medicine: Principles and Practice. 5th ed. Philadelphia, PA: Elsevier; 2020:chap 47.
Namdari S. Rotator cuff repair: tear classification, operative techniques, and outcomes. In: Matsen FA, Cordasco FA, Sperling JW, et al, eds. Rockwood and Matsen's The Shoulder. 6th ed. Philadelphia, PA: Elsevier; 2022:chap 54.
Phillips BB, Brolin TJ. Arthroscopy of the upper extremity. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 52.


, the tendon is repaired with sutures. If the tendon is separated from the bone, small rivets called suture anchors are used to attach the tendon back to the bone.</p>")

Review Date: 4/24/2023

 All rights reserved.
All rights reserved.