
Radical prostatectomy
Prostatectomy - radical; Radical retropubic prostatectomy; Radical perineal prostatectomy; Laparoscopic radical prostatectomy; LRP; Robotic-assisted laparoscopic prostatectomy; RALP; Pelvic lymphadenectomy; Prostate cancer - prostatectomy; Prostate removal - radical
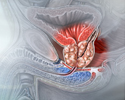
Radical prostatectomy (prostate removal) is surgery to remove all of the prostate gland and some of the tissue around it. It is done to treat prostate cancer.
Description
There are 4 main types or techniques of radical prostatectomy surgery. These procedures take about 2 to 4 hours:
- Retropubic -- Your surgeon will make a cut starting just below your belly button that reaches to your pubic bone. This surgery takes 90 minutes to 4 hours.
- Laparoscopic -- Your surgeon makes several small cuts instead of one big cut. Long, thin tools are placed inside the cuts. The surgeon puts a thin tube with a video camera (laparoscope) inside one of the cuts. This allows your surgeon to see inside your belly during the procedure.
- Robotic surgery -- Laparoscopic surgery is performed using a robotic system. Your surgeon moves the instruments and camera using robotic arms while sitting at a control console near the operating table. Not every hospital offers robotic surgery.
- Perineal -- Your surgeon makes a cut in the skin between your anus and the base of the scrotum (the perineum). The cut is smaller than with the retropubic technique. This type of surgery often takes less time and causes less loss of blood. However, it is harder for your surgeon to avoid damaging the nerves around the prostate or to remove nearby lymph nodes with this technique. This surgery is rarely done.
For these procedures, you may have general anesthesia so that you are asleep and pain free. Or, you will get medicine to numb the lower half of your body (spinal or epidural anesthesia).
- Your surgeon removes the prostate gland from the surrounding tissue. The seminal vesicles, two small fluid-filled sacs next to your prostate, are also removed.
- Your surgeon will take care to cause as little damage as possible to the nerves and blood vessels.
- Your surgeon reattaches the urethra to a part of the bladder called the bladder neck. The urethra is the tube that carries urine from the bladder out through the penis.
- Your surgeon may also remove lymph nodes in the pelvis to check them for cancer.
- A drain, called a Jackson-Pratt drain, may be left in your belly to drain extra fluid after surgery.
- A tube (catheter) is left in your urethra and bladder to drain urine. This will stay in place for a few days to a few weeks.
Why the Procedure Is Performed
Radical prostatectomy is most often done when the cancer has not spread beyond the prostate gland. This is called localized prostate cancer.
Your health care provider may recommend one treatment for you because of what is known about your type of cancer and your risk factors. Or, your provider may talk with you about other treatments that could be good for your cancer. These treatments may be used instead of surgery or after surgery has been performed.
Factors to consider when choosing a type of surgery include your age and other medical problems. Radical prostatectomy is often done on healthy men who are expected to live for 10 or more years after the procedure.
Risks
Risks of this procedure are:
- Problems controlling urine (urinary incontinence)
- Erection problems (impotence)
- Injury to the rectum
- Urethral stricture (tightening of the urinary opening due to scar tissue)
Before the Procedure
You may have several visits with your provider. You will have a complete physical exam and may have other tests. Your provider will make sure medical problems such as diabetes, high blood pressure, and heart or lung problems are under control.
If you smoke, you should stop several weeks before the surgery. Your provider can help.
Always tell your provider what medicines, vitamins, and other supplements you are taking, even ones you bought without a prescription.
During the weeks before your surgery:
- You may be asked to stop taking aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), vitamin E, clopidogrel (Plavix), warfarin (Coumadin), and any other blood thinners or medicines that make it hard for your blood to clot.
- Ask which medicines you should still take on the day of your surgery.
- On the day before your surgery, drink only clear fluids.
- Sometimes, you may be asked by your provider to take a special laxative on the day before your surgery. This will clean the contents out of your colon.
On the day of your surgery:
- Do not eat or drink anything after midnight the night before your surgery.
- Take the medicines you have been told to take with a small sip of water.
- You will be told when to arrive at the hospital. Be sure to arrive on time.
Prepare your home for when you come home after the surgery.
After the Procedure
Most people stay in the hospital for 1 to 4 days. After laparoscopic or robotic surgery, you may go home the day after the procedure.
You may need to stay in bed until the morning after surgery. You will be encouraged to move around as much as possible after that.
Your nurse will help you change positions in bed and show you exercises to keep blood flowing. You will also learn coughing or deep breathing to prevent pneumonia. You should do these steps every 1 to 2 hours. You may need to use a breathing device called an incentive spirometer to keep your lungs clear.
After your surgery, you may:
- Wear special stockings on your legs to prevent blood clots.
- Receive pain medicine in your veins or take pain pills.
- Feel spasms in your bladder.
- Have a Foley catheter in your bladder when you return home.
Outlook (Prognosis)
The surgery should remove all of the cancer cells. However, you will be monitored carefully to make sure the cancer does not come back. You should have regular checkups, including prostate specific antigen (PSA) blood tests.
Depending on the pathology results and PSA test results after prostate removal, your provider may discuss radiation therapy or hormone therapy with you.
References
Costello AJ. Considering the role of radical prostatectomy in 21st century prostate cancer care. Nat Rev Urol. 2020;17(3):177-188. PMID: 32086498 pubmed.ncbi.nlm.nih.gov/32086498/.
Li-Ming S, Otto BJ, Costello AJ. Laparoscopic and robotic-assisted laparoscopic radical prostatectomy and pelvic lymphadenectomy. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 156.
National Cancer Institute website. Prostate cancer treatment (PDQ) - health professional version. www.cancer.gov/types/prostate/hp/prostate-treatment-pdq. Updated March 11, 2024. Accessed March 27, 2024.
Schaeffer EM, Partin AW, Lepor H. Open radical prostatectomy. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 155.
Review Date: 1/1/2023
Reviewed By: Kelly L. Stratton, MD, FACS, Associate Professor, Department of Urology, University of Oklahoma Health Sciences Center, Oklahoma City, OK. Internal review and update on 01/31/2024 by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.