
Episiotomy
Labor - episiotomy; Vaginal delivery - episiotomy
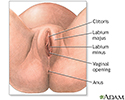
An episiotomy is a minor surgery that widens the opening of the vagina during childbirth. It is a cut to the perineum -- the skin and muscles between the vaginal opening and anus.
What are the Risks?
There are some risks to having an episiotomy. Because of the risks, episiotomies are not as common as they used to be. The risks include:
- The cut may tear and become larger during the delivery. The tear may reach into the muscle around the rectum, or even into the rectum itself.
- There may be more blood loss.
- The cut and the stitches may get infected.
- Sex may be painful for the first few months after birth.
Sometimes, an episiotomy can be helpful even with the risks.
Will I Need an Episiotomy?
Many women get through childbirth without tearing the tissue around the vagina on their own, and without needing an episiotomy. In fact, recent studies show that not having an episiotomy is best for most women in labor.
Episiotomies don't heal better than tears. They often take longer to heal since the cut is often deeper than a natural tear. In both cases, the cut or tear must be stitched and properly cared for after childbirth. At times, an episiotomy may be needed to ensure the best outcome for you and your baby such as when:
- Labor is stressful for the baby and the pushing phase needs to be shortened to decrease problems for the baby.
- The baby's head or shoulders are too big for the mother's vaginal opening.
- The baby is in a breech position (feet or buttocks coming first) and there is a problem during delivery.
- Instruments (forceps or vacuum extractor) are needed to help get the baby out.
- You are pushing as the baby's head is close to coming out, and a tear forms toward the urethral area.
What Happens if I Need an Episiotomy?
Just before your baby is born and as the head is about to crown, your doctor or midwife will give you a shot to numb the area (if you have not already had an epidural).
Next, a small incision (cut) is made. There are 2 types of cuts: median and mediolateral.
- A median incision is the most common type. It is a straight cut in the middle of the area between the vagina and anus (perineum).
- The mediolateral incision is made at an angle. It is less likely to tear through to the anus, but it takes longer to heal than the median cut.
Your doctor or midwife will then deliver the baby through the enlarged opening.
Next, your doctor or midwife will deliver the placenta (afterbirth). Then the cut will be stitched closed.
How can I Avoid an Episiotomy?
You can do things to strengthen your body for labor that may lower your chances of needing an episiotomy.
- Practice Kegel exercises.
- Perform perineal massage during the 4 to 6 weeks before birth.
- Practice the techniques you learned in childbirth class to control your breathing and your urge to push.
Keep in mind, even if you do these things, you may still need an episiotomy. Your doctor or midwife will decide if you should have one based on what happens during your labor.
References
Baggish MS. Episiotomy. In: Baggish MS, Karram MM, eds. Atlas of Pelvic Anatomy and Gynecologic Surgery. 5th ed. Philadelphia, PA: Elsevier; 2021:chap 78.
Kilpatrick SJ, Garrison E, Fairbrother E. Normal labor and delivery. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 8th ed. Philadelphia, PA: Elsevier; 2021:chap 11.

 and there is a problem during delivery. Just before the baby is born and while the woman is awake and pain-free (local anesthesia or epidural block), an incision is made at the bottom of the vaginal opening to enlarge it for the delivery of the baby's head.</p>")
 are used to close the incision after both the baby and placenta have been delivered. The stitches are absorbed by the body and do not need to be removed.</p>")
Review Date: 5/14/2024
Reviewed By: John D. Jacobson, MD, Professor Emeritus, Department of Obstetrics and Gynecology, Loma Linda University School of Medicine, Loma Linda, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.