
Systemic lupus erythematosus
Disseminated lupus erythematosus; SLE; Lupus; Lupus erythematosus; Butterfly rash - SLE; Discoid lupus
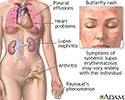
Systemic lupus erythematosus (SLE) is an autoimmune disease. In this disease, the immune system of the body mistakenly attacks healthy tissue. It can affect the skin, joints, kidneys, brain, and other organs.

Causes
The cause of SLE is not clearly known. It may be linked to the following factors:
- Genetic
- Environmental
- Hormonal
- Certain medicines
SLE is more common in women than men by nearly 10 to 1. It may occur at any age. However, it appears most often in young women between the ages of 15 and 44. In the US, the disease is more common in African Americans, Asian Americans, African Caribbeans, and Hispanic Americans.
Symptoms
Symptoms vary from person to person, and may come and go. Everyone with SLE has joint pain and swelling at some time. Some develop arthritis. SLE often affects the joints of the fingers, hands, wrists, and knees.


Other common symptoms include:
- Chest pain when taking a deep breath.
- Fatigue.
- Fever with no other cause.
- General discomfort, uneasiness, or ill feeling (malaise).
- Hair loss.
- Weight loss.
- Mouth sores.
- Sensitivity to sunlight.
- Skin rash -- A "butterfly" rash develops in about half the people with SLE. The rash is mostly seen over the cheeks and bridge of the nose. It can be widespread. It gets worse in sunlight.
- Swollen lymph nodes.





Other symptoms and signs depend on which part of the body is affected:
- Brain and nervous system -- Headaches, weakness, numbness, tingling, seizures, vision problems, memory and personality changes
- Digestive tract -- Abdominal pain, nausea, and vomiting
- Heart -- Valve problems, inflammation of heart muscle or heart lining (pericardium)
- Lung -- Buildup of fluid in the pleural space, difficulty breathing, coughing up blood
- Skin -- Sores in the mouth
- Kidney -- Swelling in the legs
- Circulation -- Clots in veins or arteries, inflammation of blood vessels, constriction of arteries in response to cold (Raynaud phenomenon)
- Blood abnormalities including anemia, low white blood cell or platelet count





Some people have only skin symptoms. This is called discoid lupus.

Exams and Tests
The American and European Rheumatology societies have published classification criteria to assist the diagnosis of SLE. These include specific symptoms, physical finding and laboratory tests. Nearly all people with SLE have a positive test for antinuclear antibody (ANA). However, having a positive ANA alone does not mean you have SLE.
The health care provider will do a complete physical exam. You may have a rash, arthritis, or swelling in the ankles. There may be an abnormal sound called a heart friction rub or pleural friction rub. Your provider will also do a nervous system exam.
Tests used to diagnose SLE may include:
- Antinuclear antibody (ANA)
- Complete blood count (CBC) with differential
- Chest x-ray
- Serum creatinine
- Urinalysis



You may also have other tests to learn more about your condition. Some of these are:
- Antinuclear antibody (ANA) panel
- Complement components (C3 and C4)
- Antibodies to double-stranded DNA
- Coombs test -- direct
- Cryoglobulins
- Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
- Kidney function blood tests
- Liver function blood tests
- Rheumatoid factor
- Antiphospholipid antibodies and lupus anticoagulant test
- Kidney biopsy
- Imaging tests of the heart, brain, lungs, joints, muscles or intestines


Treatment
There is no cure for SLE. The goal of treatment is to control symptoms. Severe symptoms that involve the heart, lungs, kidneys, and other organs often need treatment by specialists. Each person with SLE needs evaluation regarding:
- How active the disease is
- What part of the body is affected
- What form of treatment is needed
Mild forms of the disease may be treated with:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) for joint symptoms and pleurisy. Talk to your provider before taking these medicines.
- Low doses of corticosteroids, such as prednisone, for skin and arthritis symptoms.
- Corticosteroid creams for skin rashes.
- Hydroxychloroquine, a medicine also used to treat malaria.
- Methotrexate may be used to reduce the dose of corticosteroids.
- Belimumab and anifrolumab are biologic medicines that may be helpful in some people.
Treatments for more severe SLE may include:
- High-dose corticosteroids.
- Immunosuppressive medicines (these medicines suppress the immune system). These medicines are used if you have severe SLE that is affecting your nervous system, kidney, or other organs. They may also be used if you do not get better with corticosteroids, or if your symptoms get worse when you stop taking corticosteroids.
- Medicines most commonly used include mycophenolate, azathioprine, cyclophosphamide, and valcosporin. Because of its toxicity, cyclophosphamide is limited to a short course of 3 to 6 months. Rituximab (Rituxan) is used in some cases as well.
- Blood thinners, such as warfarin (Coumadin), for clotting disorders such as antiphospholipid syndrome.
If you have SLE, it is also important to:
- Wear protective clothing, sunglasses, and sunscreen when in the sun.
- Get preventive heart care.
- Stay up-to-date with immunizations.
- Have tests to screen for thinning of the bones (osteoporosis).
- Avoid tobacco and drink minimal amounts of alcohol.

Support Groups
Counseling and support groups may help with the emotional issues involved with the disease.
Outlook (Prognosis)
The outcome for people with SLE has improved in recent years. Many people with SLE have mild symptoms. How well you do depends on how severe the disease is. Most people with SLE will require medicines for a long time. Nearly all will require hydroxychloroquine indefinitely. However, in the United States, SLE is one of the top 20 leading causes of death in females between the ages of 5 and 64. Many new medicines are being studied to improve the outcome of women with SLE.
The disease tends to be more active:
- During the first years after diagnosis
- In people younger than 40 years
Many women with SLE can get pregnant and deliver a healthy baby. A good outcome is more likely for women who receive proper treatment and do not have serious heart or kidney problems. However, the presence of certain SLE antibodies or antiphospholipid antibodies raises the risk of miscarriage.
Possible Complications
LUPUS NEPHRITIS
Some people with SLE have abnormal immune deposits in the kidney cells. This leads to a condition called lupus nephritis. People with this problem may develop kidney failure. They may need dialysis or a kidney transplant.
A kidney biopsy is done to detect the extent of damage to the kidney and to help guide treatment. If active nephritis is present, treatment with immunosuppressive medicines including high doses of corticosteroids along with either cyclophosphamide or mycophenolate are needed.
OTHER PARTS OF THE BODY
SLE can cause damage in many different parts of the body, including:
- Blood clots in arteries or veins of the legs, lungs, brain, or intestines
- Destruction of red blood cells or anemia of long-term (chronic) disease
- Fluid around the heart (pericarditis), or inflammation of the heart (myocarditis or endocarditis)
- Fluid around the lungs (pleuritis) and damage to lung tissue
- Pregnancy problems, including miscarriage
- Stroke
- Bowel damage with abdominal pain and obstruction
- Inflammation in the intestines
- Severely low blood platelet count (platelets are needed to stop any bleeding)
- Inflammation of the blood vessels






SLE AND PREGNANCY
Both SLE and some of the medicines used for SLE can harm an unborn child. Talk to your provider before you become pregnant. If you become pregnant, find a provider who is experienced with SLE and pregnancy.
When to Contact a Medical Professional
Contact your provider if you have symptoms of SLE. Also contact your provider if you have this disease and your symptoms get worse or a new symptom occurs.
References
Aringer M, Costenbader K, Daikh D, et al. 2019 European League against rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. 2019;71(9):1400-1412. PMID: 31385462 pubmed.ncbi.nlm.nih.gov/31385462/.
Crow MK. Etiology and pathogenesis of systemic lupus erythematosus. In: Firestein GS, Budd RC, Gabriel SE, Koretzky GA, McInnes IB, O'Dell JR, eds. Firestein & Kelley's Textbook of Rheumatology. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 84.
Crow MK. Systemic lupus erythematosus. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 245.
Fanouriakis A, Kostopoulou M, Alunno A, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019;78(6):736-745. PMID: 30926722 pubmed.ncbi.nlm.nih.gov/30926722/.
Systemic lupus erythematosus - illustration
Systemic lupus erythematosus
illustration
Lupus, discoid - view of lesions on the chest - illustration
Lupus, discoid - view of lesions on the chest
illustration
Lupus - discoid on a child's face - illustration
Lupus - discoid on a child's face
illustration
Systemic lupus erythematosus rash on the face - illustration
Systemic lupus erythematosus rash on the face
illustration
Antibodies - illustration
Antibodies
illustration




Systemic lupus erythematosus - illustration
Systemic lupus erythematosus
illustration
Lupus, discoid - view of lesions on the chest - illustration
Lupus, discoid - view of lesions on the chest
illustration
Lupus - discoid on a child's face - illustration
Lupus - discoid on a child's face
illustration
Systemic lupus erythematosus rash on the face - illustration
Systemic lupus erythematosus rash on the face
illustration
Antibodies - illustration
Antibodies
illustration
Review Date: 1/25/2023
Reviewed By: Neil J. Gonter, MD, Assistant Professor of Medicine, Columbia University, NY and private practice specializing in Rheumatology at Rheumatology Associates of North Jersey, Teaneck, NJ. Review provided by VeriMed Healthcare Network. Internal review and update on 01/25/2024 by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.