
Intussusception – children
Abdominal pain in children - intussusception
Intussusception is the sliding of one part of the intestine into another.
This article focuses on intussusception in children.
Causes
Intussusception is caused by part of the intestine being pulled inward into itself.
The pressure created by the walls of the intestine pressing together causes:
- Decreased blood flow
- Irritation
- Swelling
Intussusception can block the passage of food through the intestine. If the blood supply is cut off, the segment of intestine pulled inside can die. Heavy bleeding may also occur. If a hole develops, infection, shock, and dehydration can take place very rapidly.


The cause of intussusception is not known. Conditions that may lead to the problem include:
- Viral infection
- Enlarged lymph node in the intestine
- Polyp or tumor in the bowel
Intussusception can affect both children and adults. It is more common in boys. It usually affects children ages 5 months to 3 years.
Symptoms
The first sign of intussusception is very often sudden, loud crying caused by abdominal pain. The pain is colicky and not continuous (intermittent), but it comes back often. The pain will get stronger and last longer each time it returns.

An infant with severe abdominal pain may draw the knees to the chest while crying.
Other symptoms include:
- Bloody, mucus-like bowel movement, sometimes called a "currant jelly" stool
- Fever
- Shock (pale color, lethargy, sweating)
- Stool mixed with blood and mucus
- Vomiting
Exams and Tests
Your health care provider will perform a thorough exam, which may reveal a mass in the abdomen. There may also be signs of dehydration or shock.

Tests may include:
- Abdominal ultrasound
- Abdominal x-ray
- Air or contrast enema


Treatment
The child will first be stabilized. A tube will be passed into the stomach through the nose (nasogastric tube). An intravenous (IV) line will be placed in the arm, and fluids will be given to prevent dehydration.
In some cases, the bowel blockage can be treated with an air or contrast enema. This is done by a radiologist skilled with the procedure. There is a risk of bowel tearing (perforation) with this procedure.

The child will need surgery if these treatments do not work. The bowel tissue can very often be saved. Dead tissue will be removed.
Antibiotics may be needed to treat any infection.
Intravenous feeding and fluids will be continued until the child has a normal bowel movement.
Outlook (Prognosis)
The outcome is good with early treatment. There is a risk this problem will come back.
When a hole or tear in the bowel occurs, it must be treated right away. If not treated, intussusception is almost always fatal for infants and young children.
When to Contact a Medical Professional
Intussusception is a medical emergency. Call 911 or the local emergency number, or go to the emergency room right away.
References
Abdulhai S, Ponsky T. Intussusception in infants and children. In: Wyllie R, Hyams JS, Kay M, eds. Pediatric Gastrointestinal and Liver Disease. 6th ed. Philadelphia, PA: Elsevier; 2021:chap 51.
Hu YY, Jensen T, Finck C. Surgical conditions of the small intestine in infants and children. In: Yeo CJ, ed. Shackelford's Surgery of the Alimentary Tract. 8th ed. Philadelphia, PA: Elsevier; 2019:chap 83.
Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM. Ileus, adhesions, intussusception, and closed-loop obstructions. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 359.
Maloney PJ. Pediatric gastrointestinal disorders. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 166.
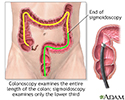
Colonoscopy - illustration
Colonoscopy
illustration
Intussusception - X-ray - illustration
Intussusception - X-ray
illustration
Digestive system organs - illustration
Digestive system organs
illustration


Review Date: 2/17/2024
Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.