
Heart bypass surgery - minimally invasive
Minimally invasive direct coronary artery bypass; MIDCAB; Robot-assisted coronary artery bypass; RACAB; Keyhole heart surgery; CAD - MIDCAB; Coronary artery disease - MIDCAB
Heart bypass surgery creates a new route, called a bypass, for blood and oxygen to reach your heart.
Minimally invasive coronary (heart) artery bypass can be done without stopping the heart. Therefore, you do not need to be put on a heart-lung machine for this procedure.
Description
To perform this surgery:
- The heart surgeon will make a 3- to 5-inch (8 to 13 centimeters) surgical cut in the left part of your chest between your ribs to reach your heart.
- Muscles in the area will be pushed apart. A small part of the front of the rib, called the costal cartilage, will be removed.
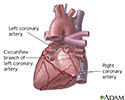
- The surgeon will then find and prepare an artery on your chest wall (internal mammary artery) to attach to your coronary artery that is blocked.
- Next, the surgeon will use sutures to connect the prepared chest artery to the coronary artery that is blocked.
You will not be on a heart-lung machine for this surgery. However, you will have general anesthesia so you will be asleep and not feel pain. A device will be attached to your heart to stabilize it. You will also receive medicine to slow the heart down.
You may have a tube in your chest for drainage of fluid. This will be removed in a day or two.
Why the Procedure Is Performed
Your health care provider may recommend a minimally invasive coronary artery bypass if you have a blockage in one or two coronary arteries, most often in the front of the heart.
When one or more of the coronary arteries become partly or totally blocked, your heart does not get enough blood. This is called ischemic heart disease or coronary artery disease. It can cause chest pain (angina).
Your provider may have first tried to treat you with medicines. You may have also tried cardiac rehabilitation or other treatments, such as angioplasty with stenting.
Coronary artery disease varies from person to person. Heart bypass surgery is just one type of treatment. It is not right for everyone.
Surgeries or procedures that may be done instead of minimally invasive heart bypass are:


Risks
Your provider will talk to you about the risks of surgery. In general, the complications of minimally invasive coronary artery bypass are lower than with open coronary artery bypass surgery.
Risks related to any surgery include:
- Blood clots in the legs that may travel to the lungs
- Blood loss
- Breathing problems
- Heart attack or stroke
- Infection of the lungs, urinary tract, and chest
- Temporary or permanent brain injury
Possible risks of coronary artery bypass include:
- Memory loss, loss of mental clarity, or "fuzzy thinking." This is less common in people who have minimally invasive coronary artery bypass than in people who have open coronary bypass.
- Heart rhythm problems (arrhythmia).
- A chest wound infection. This is more likely to happen if you are obese, have diabetes, or have had coronary bypass surgery in the past.
- Low-grade fever and chest pain (together called postpericardiotomy syndrome), which can last up to 6 months.
- Pain at the site of the cut.
- Possible need to convert to conventional procedure with bypass machine during surgery.
Before the Procedure
Always tell your surgeon what medicines you are taking, even drugs or herbs you bought without a prescription.
During the days before the surgery:
- For the 2-week period before surgery, you may be asked to stop taking medicines that make it harder for your blood to clot. These might cause increased bleeding during the surgery. They include aspirin, ibuprofen (such as Advil and Motrin), naproxen (such as Aleve and Naprosyn), and other similar drugs. If you are taking clopidogrel (Plavix), ask your surgeon when you should stop taking it before surgery.
- Ask your surgeon which medicines you should still take on the day of the surgery.
- If you smoke, try to stop. Ask your provider for help.
- Contact your provider if you have a cold, flu, fever, herpes breakout, or any other illness.
- Prepare your home so you can move around easily when you return from the hospital.

The day before your surgery:
- Shower and shampoo well.
- You may be asked to wash your whole body below your neck with a special soap. Scrub your chest 2 or 3 times with this soap.
On the day of the surgery:
- You will most often be asked not to drink or eat anything after midnight the night before your surgery. This includes chewing gum and using breath mints. Rinse your mouth with water if it feels dry, but be careful not to swallow.
- Take the medicines your surgeon told you to take with a small sip of water.
Your surgeon will tell you when to arrive at the hospital.
After the Procedure
You may be able to leave the hospital 2 or 3 days after your surgery. The surgeon or nurse will tell you how to care for yourself at home. You may be able to return to normal activities after 2 or 3 weeks.

Outlook (Prognosis)
Recovery from surgery takes time, and you may not see the full benefits of your surgery for 3 to 6 months. In most people who have heart bypass surgery, the grafts remain open and work well for many years.
This surgery does not prevent a blockage from coming back. However, you can take steps to slow it down. Things you can do include:
- Do not smoke.
- Eat a heart-healthy diet.
- Get regular exercise.
- Treat high blood pressure, high blood sugar (if you have diabetes), and high cholesterol.
You may be more likely to have problems with your blood vessels if you have kidney disease or other medical problems.
References
Omer S, Bakaeen FG. Acquired heart disease: coronary insufficiency. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. Philadelphia, PA: Elsevier; 2022:chap 60.
Qureshi SH, Guo MH, Ruel M.. Less -invasive and robotic approaches to coronary artery bypass grafting. In: Sellke FW, del Nido PJ, Swanson SJ, eds. Sabiston and Spencer Surgery of the Chest. 10th ed. Philadelphia, PA: Elsevier; 2024:chap 94.. 2nd ed. Philadelphia, PA: Elsevier; 2019:chap 5.
Rodriguez ML, Ruel M. Minimally invasive coronary artery bypass grafting. In: Sellke FW, Ruel M, eds. Atlas of Cardiac Surgical Techniques. 2nd ed. Philadelphia, PA: Elsevier; 2019:chap 5.
Writing Committee Members; Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79 (2):e21-e129. PMID: 34895950 pubmed.ncbi.nlm.nih.gov/34895950/.
Heart - front view - illustration
Heart - front view
illustration
Posterior heart arteries - illustration
Posterior heart arteries
illustration
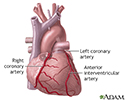
Anterior heart arteries - illustration
Anterior heart arteries
illustration
Coronary artery stent - illustration
Coronary artery stent
illustration
Heart bypass surgery - series - Normal anatomy
Presentation
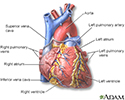



 or heart bypass surgery is recommended when one or more coronary arteries are seriously blocked and blood supply to the heart muscle is insufficient. Several tests are done to identify the cause of the chest pain (angina), such as blood tests and x-ray studies (angiograms).</p>")

. It is done through an opening through the breast bone. While one surgeon is working on the chest, another surgeon works on taking a length of vein (saphenous vein) for the bypass through a long incision along the inside of the lower leg. The vein is sewn in above and below the blockage in the coronary artery. Alternatively, an artery from the interior aspect of the chest wall (internal mammary artery), or the arm (radial artery) is used.</p>")

. Chest tubes will be in place for the first 2 to 3 days to drain any residual blood and fluid from around the heart. Heart functions will be monitored. The full benefits from the operation may not be ascertained until 3 to 6 months after surgery. Sexual activity may be resumed 3 to 4 weeks after surgery. All activities that do not cause fatigue are permitted, but the patient must not strain the healing chest bone (sternum).</p>")
Heart - front view - illustration
Heart - front view
illustration
Posterior heart arteries - illustration
Posterior heart arteries
illustration
Anterior heart arteries - illustration
Anterior heart arteries
illustration
Coronary artery stent - illustration
Coronary artery stent
illustration
Heart bypass surgery - series - Normal anatomy
Presentation
Review Date: 5/13/2024
Reviewed By: Mary C. Mancini, MD, PhD, Cardiothoracic Surgeon, Shreveport, LA. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.