
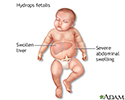
Hydrops fetalis
Hydrops fetalis is a serious condition. It occurs when abnormal amounts of fluid build up in two or more body areas of a fetus or newborn. It is a symptom of underlying problems.
There are two types of hydrops fetalis, immune and nonimmune. The type depends on the cause of the abnormal fluid.
- Immune hydrops fetalis is most often a complication of a severe form of Rh incompatibility, which can be prevented. This is a condition in which mother who has Rh negative blood type makes antibodies to her baby's Rh positive blood cells, and the antibodies cross the placenta. Rh incompatibility causes a large number of red blood cells in the fetus to be destroyed (also known as hemolytic disease of the newborn). This leads to problems including total body swelling. Severe swelling can interfere with how the body organs work.
- Nonimmune hydrops fetalis is more common. It accounts for up to 90% of cases of hydrops. The condition occurs when a disease or medical condition affects the body's ability to manage fluid. There are three main causes for this type, heart or lung problems, severe anemia (such as from thalassemia or infections), and genetic or developmental problems, including Turner syndrome.



The number of babies who develop immune hydrops fetalis has dropped due to a medicine called RhoGAM. This drug is given as an injection to pregnant mothers who are at risk for Rh incompatibility. The drug prevents them from making antibodies against their babies' red blood cells. There are other, much rarer, blood group incompatibilities that can also cause immune hydrops fetalis, but RhoGAM does not help with these.
Symptoms
Symptoms depend on the severity of the condition. Mild forms may cause:
- Liver swelling
- Change in skin color (pallor)
More severe forms may cause:
- Breathing problems
- Bruising or purplish bruise-like spots on the skin
- Heart failure
- Severe anemia
- Severe jaundice
- Total body swelling
Exams and Tests
An ultrasound done during pregnancy may show:
- High levels of amniotic fluid
- Abnormally large placenta
- Fluid causing swelling in and around the unborn baby's organs, including the liver, spleen, heart, or lung area
An amniocentesis and frequent ultrasounds will be done to determine the severity of the condition.
Treatment
Treatment depends on the cause. During pregnancy, treatment may include:
- Medicine to cause early labor and delivery of the baby
- Early cesarean delivery if condition gets worse
- Giving blood to the baby while still in the womb (intrauterine fetal blood transfusion)
Treatment for a newborn may include:
- For immune hydrops, direct transfusion of red blood cells that match the infant's blood type. An exchange transfusion to rid the baby's body of the substances that are destroying the red blood cells may also be done.
- Removing extra fluid from around the lungs and abdominal organs with a needle.
- Medicines to control heart failure and help the kidneys remove extra fluids.
- Methods to help the baby breathe, such as a breathing machine (ventilator).
Outlook (Prognosis)
Hydrops fetalis often results in death of the infant shortly before or after delivery. The risk is highest for babies who are born very early or who are ill at birth. Babies who have a structural defect, and those with no identified cause for the hydrops are also at higher risk.
Possible Complications
Brain damage called kernicterus may occur in the case of Rh incompatibility. Developmental delays have been seen in babies who received intrauterine transfusions.

Prevention
Rh incompatibility can be prevented if the mother is given RhoGAM during and after pregnancy.
References
Langlois S, Wilson RD. Fetal hydrops. In: Pandya PP, Oepkes D, Sebire NJ, Wapner RJ, eds. Fetal Medicine: Basic Science and Clinical Practice. 3rd ed. Philadelphia, PA: Elsevier; 2020:chap 36.
Simmons PM, Magann EF. Immune and nonimmune hydrops fetalis. In: Martin RJ, Fanaroff AA, Walsh MC, eds. Fanaroff and Martin's Neonatal-Perinatal Medicine. 11th ed. Philadelphia, PA: Elsevier; 2020:chap 23.
Suhrie KR, Tabbah SM. High-risk pregnancies. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 114.
Review Date: 4/25/2023
Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.