
Esophagectomy - open
Trans-hiatal esophagectomy; Trans-thoracic esophagectomy; En bloc esophagectomy; Removal of the esophagus - open; Ivor-Lewis esophagectomy, Blunt esophagectomy; Esophageal cancer - esophagectomy - open; Cancer of the esophagus - esophagectomy - open
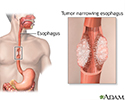
Open esophagectomy is surgery to remove part or all of the esophagus. This is the tube that moves food from your throat to your stomach. After it is removed, the esophagus is rebuilt from part of your stomach or part of your large intestine.
Most of the time, esophagectomy is done to treat cancer of the esophagus or a severely damaged esophagus.

Description
During open esophagectomy, one or more large surgical cuts (incisions) are made in your belly, chest, or neck. (Another way to remove the esophagus is laparoscopically. Surgery is done through several small incisions, using a viewing scope.)

This article discusses three types of open surgery. With any surgery, you will receive medicine (anesthesia) that will keep you asleep and pain-free.
Transhiatal esophagectomy:
- The surgeon makes two large cuts. One cut is in your neck area and one is in your upper belly.
- From the cut in the belly, the surgeon frees the stomach and lower part of the esophagus from the nearby tissues. From the cut in the neck, the rest of the esophagus is freed.
- The surgeon then removes the part of your esophagus where the cancer or other problem is.
- Your stomach is then reshaped into a tube to make a new esophagus. It is joined to the remaining part of your esophagus with staples or stitches.
- During surgery, lymph nodes in your neck and belly are likely removed to determine if cancer has spread to them.
- A feeding tube is placed in your small intestine so that you can be fed while you are recovering from surgery.
- Drainage tubes may be left in the chest to remove fluid.
Transthoracic esophagectomy: This surgery is done in a similar way as the transhiatal procedure. But the upper cut is made in your right chest, not in the neck.
En bloc esophagectomy:
- The surgeon makes large cuts in your neck, chest, and belly. All of your esophagus and part of your stomach are removed.
- The rest of your stomach is reshaped into a tube and placed in your chest to replace your esophagus. The stomach tube is connected to the remaining esophagus in the neck.
- The surgeon also removes all lymph nodes in your chest, neck, and belly.
Most of these operations take 3 to 6 hours.
Why the Procedure Is Performed
Surgery to remove the lower esophagus may also be done to treat:
- A condition in which the ring of muscle in the esophagus does not work well (achalasia)
- Severe damage of the lining of the esophagus that can lead to cancer (Barrett esophagus)
- Severe trauma
- Destroyed esophagus
- Severely damaged stomach
Risks
This is major surgery and has many risks. Some of them are serious. Be sure to discuss these risks with your surgeon.
Risks of this surgery, or for problems after surgery, may be greater than normal if you:
- Are unable to walk, even for short distances (this increases the risk of blood clots, lung problems, and pressure sores)
- Are older than 60 years
- Are a heavy smoker
- Are obese
- Have lost a lot of weight from your cancer
- Are on steroid medicines
- Have had a severe infection from the damaged esophagus/stomach
- Received cancer drugs (chemotherapy) before the surgery
Risks for anesthesia and surgery in general are:
- Allergic reactions to medicines
- Breathing problems
- Bleeding, blood clots, or infection


Risks for this surgery are:
- Acid reflux
- Injury to the stomach, intestines, lungs, or other organs during surgery
- Leakage of the contents of your esophagus or stomach where the surgeon joined them together
- Narrowing of the connection between your stomach and esophagus
- Pneumonia
- Difficulty swallowing or speaking
- Bowel obstruction
Before the Procedure
You will have many medical visits and tests before surgery, including:
- A complete physical examination.
- Visits with your health care provider to make sure other medical problems you may have, such as diabetes, high blood pressure, and heart or lung problems are under control.
- Nutritional counseling.
- A visit or class to learn what happens during surgery, what you should expect afterward, and what risks or problems may occur afterward.
- If you have recently lost weight, your doctor may put you on oral or IV nutrition for several weeks before surgery.
- CT scan to look at the esophagus.
- PET scan to identify the cancer and if it has spread.
- Endoscopy to diagnose and identify how far the cancer has spread.




If you are a smoker, you should stop smoking several weeks before surgery. Your provider can help.
Tell your provider:
- If you are or might be pregnant
- What medicines, vitamins, and other supplements you are taking, even ones you bought without a prescription
- If you have been drinking a lot of alcohol, more than 1 or 2 drinks a day
During the week before surgery:
- You may be asked to stop taking blood thinner medicines. Some of these are aspirin, ibuprofen (Advil, Motrin), vitamin E, warfarin (Coumadin), and clopidogrel (Plavix).
- Ask your surgeon which medicines you should still take on the day of surgery.
- Prepare your home for after surgery.
On the day of surgery:
- Follow instructions on when to stop eating and drinking before surgery.
- Take the medicines your surgeon told you to take with a small sip of water.
- Arrive at the hospital on time.
After the Procedure
Most people stay in the hospital for 7 to 14 days after this surgery. You may spend 1 to 3 days in the intensive care unit (ICU) right after surgery.
During your hospital stay, you will:
- Be asked to sit on the side of your bed and walk on the same day or day after surgery.
- Not be able to eat for at least the first 5 to 7 days after surgery. After that, may be able to start with liquids. You will be fed through a feeding tube that was placed into your intestine during surgery.
- Have a tube coming out of the side of your chest to drain fluids that build up.
- Wear special stockings on your feet and legs to prevent blood clots.
- Receive shots to prevent blood clots.
- Receive pain medicine through an IV or take pills. You may receive your pain medicine through a special pump. With this pump, you press a button to deliver pain medicine when you need it. This allows you to control the amount of pain medicine you get.
- Do breathing exercises to prevent lung infection.

After you go home, follow instructions on how to take care of yourself as you heal. You'll be given information on diet and eating. Be sure to follow those instructions as well.
Outlook (Prognosis)
Many people recover well from this surgery and can have a normal diet. After they recover, they will likely have to eat smaller portions and eat more often.
If you had the surgery for cancer, talk with your provider about the next steps to treat the cancer.
References
National Cancer Institute website. Esophageal cancer treatment (PDQ) - health professional version. www.cancer.gov/types/esophageal/hp/esophageal-treatment-pdq. Updated October 14, 2022. Accessed February 28, 2023.
Rajaram R, Spicer JD, Dhupar R, Kim JY, Sepesi B, Hofstetter W. Esophagus. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. St Louis, MO: Elsevier; 2022:chap 42.
Review Date: 1/23/2023
Reviewed By: Mary C. Mancini, MD, PhD, Cardiothoracic Surgeon, Shreveport, LA. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.