
Cystinuria
Stones - cystine; Cystine stones
Cystinuria is a rare condition in which stones made from an amino acid called cysteine form in the kidney, ureter, or bladder. Cystine is formed when two molecules of an amino acid called cysteine are bound together. The condition is passed down through families.

Causes
To have the symptoms of cystinuria, you must inherit a variant gene from both parents. Your children will also inherit a copy of the variant gene from you.
Cystinuria is caused by too much cystine in the urine. Normally, most cystine dissolves and returns to the bloodstream after entering the kidneys. People with cystinuria have a genetic change that interferes with this process. As a result, cystine builds up in the urine and forms crystals or stones. These crystals may get stuck in the kidneys, ureters, or bladder.
About one in every 7000 people have cystinuria. Cystine stones are most common in young adults under age 40. Less than 3% of urinary tract stones are cystine stones.

Symptoms
Symptoms include:
- Blood in the urine
- Flank pain or pain in the side or back. Pain is most often on one side. It is rarely felt on both sides. Pain is often severe. It may get worse over days. You may also feel pain in the pelvis, groin, genitals, or between the upper abdomen and back.

Exams and Tests
The condition is most often diagnosed after an episode of kidney stones. Testing the stones after they are removed shows that they are made of cystine.
Unlike calcium-containing stones, cystine stones do not show up well on plain x-rays.
Tests that may be done to detect these stones and diagnose the condition include:



Treatment
The goal of treatment is to relieve symptoms and prevent more stones from forming. A person with severe symptoms may need to go into the hospital.
Treatment involves drinking plenty of fluids, especially water, to produce large amounts of urine. You should drink at least 6 to 8 glasses per day. You should drink water at night as well so that you get up at night at least once to pass urine.
In some cases, fluids may need to be given through a vein (by IV).
Making the urine more alkaline may help dissolve the cystine crystals. This may be done with use of potassium citrate or sodium bicarbonate. Eating less salt can also decrease cystine release and stone formation.
You may need pain relievers to control pain in the kidney or bladder area when you pass stones. Smaller stones (5 mm or less in diameter) most often pass through the urine on their own. Larger stones (more than 5 mm) may need extra treatments. Some large stones may need to be removed using procedures such as:
- Extracorporeal shock wave lithotripsy (ESWL): Sound waves are passed through the body and are focused on the stones to break them into small, passable fragments. ESWL may not work well for cystine stones because they are very hard as compared with other types of stones.
- Percutaneous nephrostolithotomy or nephrolithotomy: A small tube is placed through the flank directly into the kidney. A telescope is then passed through the tube to fragment the stone under direct vision.
- Ureteroscopy and laser lithotripsy: The laser is used to break up the stones and can be used to treat stones that are not too large.
Outlook (Prognosis)
Cystinuria is a chronic, lifelong condition. Without treatment, stones commonly return. However, the condition rarely results in kidney failure. It does not affect other organs.

Possible Complications
Complications may include:
- Bladder injury from stone
- Kidney injury from stone
- Kidney infection
- Chronic kidney disease
- Ureteral obstruction
- Urinary tract infection

When to Contact a Medical Professional
Contact your health care provider if you have symptoms of urinary tract stones.
Prevention
There are medicines that can be taken so cystine in the urine does not form a stone. Ask your provider about these medicines and their side effects.
Any person with a known history of stones in the urinary tract should drink plenty of fluids to regularly produce a high amount of urine. This allows stones and crystals to leave the body before they become large enough to cause symptoms. Decreasing your intake of salt or sodium will help as well.
References
Di Carlo HN, Crigger CB . Urinary lithiasis. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 584.
Guay-Woodford LM. Hereditary nephropathies and developmental renal/urinary abnormalities. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 113.
Miller NL, Borofsky MS. Evaluation and medical management of urinary lithiasis. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 92.
Sakhaee K, Moe OW. Urolithiasis. In: Yu ASL, Chertow GM, Luyckx VA, Marsden PA, Skorecki K, Taal MW, eds. Brenner and Rector's The Kidney. 11th ed. Philadelphia, PA: Elsevier; 2020:chap 38.
Kidney stones
Animation
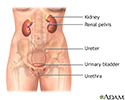
Female urinary tract - illustration
Female urinary tract
illustration
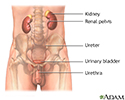
Male urinary tract - illustration
Male urinary tract
illustration
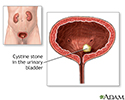
Cystinuria - illustration
Cystinuria
illustration
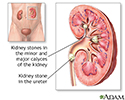
Nephrolithiasis - illustration
Nephrolithiasis
illustration

Review Date: 3/31/2024
Reviewed By: Sovrin M. Shah, MD, Associate Professor, Department of Urology, The Icahn School of Medicine at Mount Sinai, New York, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.