
Prostate cancer treatment
Treatment for your prostate cancer is chosen after a thorough evaluation. Your health care provider will discuss the benefits and risks of each treatment.

Sometimes your provider may recommend one treatment for you because of your type of cancer and risk factors. Other times, there may be two or more treatments that could be good for you.
Factors you and your provider must think about include:
- Your age and other medical problems you may have
- Side effects that occur with each type of treatment
- Whether the prostate cancer is localized or how much the prostate cancer has spread (described by the stage of the cancer)
- Your Gleason score, which tells how aggressive the cancer is
- Your prostate-specific antigen (PSA) test result

Ask your provider to explain these things following about your treatment choices:
- Which choices offer the best chance of curing your cancer or controlling its spread?
- How likely is it that you will have different side effects, and how they will affect your life?
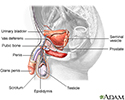
Radical prostatectomy is a surgery to remove the prostate and some of the surrounding tissue. It is an option when the cancer has not spread beyond the prostate gland.
Healthy men who will likely live 10 or more years after being diagnosed with prostate cancer often have this procedure.
Be aware that it is not always possible to know for certain, before surgery, if the cancer has spread beyond the prostate gland.
Possible problems after surgery include difficulty controlling urination and erection problems. Also, some men need further treatments after this surgery.

Radiation Therapy
Radiation therapy works best for treating prostate cancer that has not spread beyond the prostate. It may also be used after surgery if there is a risk that cancer cells are still present. Radiation is sometimes used for pain relief when cancer has spread to the bone.

External beam radiation therapy uses high-powered x-rays pointed at the prostate gland:
- Before treatment, the radiation therapist uses a special pen to mark the part of the body that is to be treated.
- Radiation is delivered to the prostate gland using a machine similar to a regular x-ray machine. The treatment itself is usually painless.
- Treatment is done in a radiation oncology center that is usually connected to a hospital.
- Treatment is usually done 5 days a week for 6 to 8 weeks.
Side effects may include:
- Appetite loss
- Diarrhea
- Erection problems
- Fatigue
- Rectal burning or injury
- Skin reactions
- Urinary incontinence, the feeling of needing to urinate urgently, or blood in the urine

There are reports of secondary cancers arising from the radiation as well.
Proton therapy is another kind of radiation therapy used to treat prostate cancer. Proton beams target the tumor precisely, so there is less damage to the surrounding tissue. This therapy is not widely accepted or used.
Prostate Brachytherapy
Brachytherapy is often used for small prostate cancers that are found early and are slow-growing. Brachytherapy may be combined with external beam radiation therapy for more advanced cancers.
Brachytherapy involves placing radioactive seeds inside the prostate gland.
- A doctor (usually a radiation oncologist) inserts small needles through the skin beneath your scrotum to inject the seeds. The seeds are so small that you do not feel them.
- The seeds are left in place permanently.
Side effects may include:
- Pain, swelling, or bruising in the penis or scrotum
- Red-brown urine or semen
- Impotence
- Incontinence
- Urinary retention
- Diarrhea
Hormonal Therapy
Testosterone is the main male hormone. Prostate tumors need testosterone to grow. Hormonal therapy is treatment that decreases the effect of testosterone on prostate cancer.
Hormone therapy is mainly used for cancer that has spread beyond the prostate, but it can also be used along with surgery and radiation to treat advanced cancers. The treatment can help relieve symptoms and prevent further growth and spread of cancer. But it does not cure the cancer.
The main type of hormone therapy is called a luteinizing hormone-releasing hormones (LH-RH) agonist. Another class of therapy is called LH-RH antagonists:
- Both types of medicines block the testicles from making testosterone. The drugs must be given by injection, usually every 3 to 6 months.
- Possible side effects include nausea and vomiting, hot flashes, breast growth and/or tenderness, anemia, fatigue, thinning bones (osteoporosis), reduced sexual desire, decreased muscle mass, weight gain, and impotence.
The other type of hormone medicine is called an androgen-blocking drug:
- It is often given along with LH-RH drugs to block the effect of testosterone produced by the adrenal glands, which make a small amount of testosterone.
- Possible side effects include erection problems, reduced sexual desire, liver problems, diarrhea, and enlarged breasts.

Much of the body's testosterone is made by the testes. As a result, surgery to remove the testes (called orchiectomy) can also be used as a hormonal treatment.
Chemotherapy
Chemotherapy and immunotherapy (medicine that helps the body's immune system fight the cancer) may be used to treat prostate cancer that no longer responds to hormone treatment. Usually a single drug or a combination of drugs is recommended.

Cryotherapy
Cryotherapy uses very cold temperatures to freeze and kill prostate cancer cells. The goal of cryosurgery is to destroy the entire prostate gland and possibly surrounding tissue.
Cryosurgery is generally not used as a first treatment for prostate cancer.
References
National Cancer Institute website. Prostate cancer treatment (PDQ) - health professional version. www.cancer.gov/types/prostate/hp/prostate-treatment-pdq. Updated February 13, 2023. Accessed January 18, 2024.
National Comprehensive Cancer Network website. NCCN clinical practice guidelines in oncology (NCCN guidelines): prostate cancer. Version 4.2023. www.nccn.org/professionals/physician_gls/pdf/prostate.pdf. Updated September 7, 2023. Accessed January 18, 2024.
Nelson WG, Antonarakis ES, Carter HB, De Marzo AM, DeWeese TL. Prostate cancer. In: Niederhuber JE, Armitage JO, Kastan MB, Doroshow JH, Tepper JE, eds. Abeloff's Clinical Oncology. 6th ed. Philadelphia, PA: Elsevier; 2020:chap 81.
Review Date: 10/15/2023
Reviewed By: Kelly L. Stratton, MD, FACS, Associate Professor, Department of Urology, University of Oklahoma Health Sciences Center, Oklahoma City, OK. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.