
Simple goiter
Goiter - simple; Endemic goiter; Colloidal goiter; Nontoxic goiter
A simple goiter is an enlargement of the thyroid gland. It is usually not a tumor or cancer.
Causes
The thyroid gland is an important organ of the endocrine system. It is located at the front of the neck just above where your collarbones meet. The gland makes the hormones that control the way every cell in the body uses energy. This process is called metabolism.


Iodine deficiency is the most common cause of goiter. The body needs iodine to produce thyroid hormone. If you do not have enough iodine in your diet, the thyroid gets larger to try and capture all the iodine it can, so it can make the right amount of thyroid hormone. So, a goiter can be a sign the thyroid is not able to make enough thyroid hormone. The use of iodized salt in the United States prevents a lack of iodine in the diet for people who use it.
Other causes of goiter include:
- The body's immune system attacking the thyroid gland (autoimmune problem)
- Certain medicines (lithium, amiodarone)
- Infections (rare)
- Cigarette smoking
- Eating very large amounts of certain foods (soy, peanuts, or vegetables in the broccoli and cabbage family)
- Toxic nodular goiter, an enlarged thyroid gland that has a small growth or many growths called nodules, which produce too much thyroid hormone


Simple goiters are more common in:
- People over age 40
- People with a family history of goiter
- People who are born and raised in areas with iodine deficiency
- Women
Symptoms
The main symptom is an enlarged thyroid gland. The size may range from a single small nodule to a large mass at the front of the neck.

Some people with a simple goiter may have symptoms of an underactive thyroid gland.

In rare cases, an enlarged thyroid can put pressure on the windpipe (trachea) and food tube (esophagus). This can lead to:
- Breathing difficulties (with very large goiters), especially when lying flat on the back or when reaching up with your arms
- Cough
- Hoarseness
- Swallowing difficulties, especially with solid food
- Pain in the area of the thyroid

Exams and Tests
Your health care provider will do a physical exam. This involves feeling your neck as you swallow. Swelling in the area of the thyroid may be felt.
If you have a very large goiter, you may have pressure on your neck veins. As a result, when your provider asks you to raise your arms above your head, you may feel dizzy.
Blood tests may be ordered to measure thyroid function:

Tests to look for abnormal and possibly cancerous areas in the thyroid gland include:


If nodules are found on an ultrasound, a biopsy may be needed to check for thyroid cancer.
Treatment
A goiter only needs to be treated if it is causing symptoms.
Treatments for an enlarged thyroid include:
- Thyroid hormone replacement pills if the goiter is due to an underactive thyroid
- Small doses of Lugol's iodine or potassium iodine solution if the goiter is due to a lack of iodine
- Radioactive iodine to shrink the gland if the thyroid is producing too much thyroid hormone
- Surgery (thyroidectomy) to remove all or part of the gland

Outlook (Prognosis)
A simple goiter may disappear on its own, or may become larger. Over time, the thyroid gland may stop making enough thyroid hormone. This condition is called hypothyroidism.
In some cases, a goiter becomes toxic and produces thyroid hormone on its own. This can cause high levels of thyroid hormone, a condition called hyperthyroidism.
When to Contact a Medical Professional
Contact your provider if you experience any swelling in the front of your neck or any other symptoms of goiter.
Prevention
Using iodized table salt prevents most simple goiters.
References
Filetti S, Tuttle RM, Leboulleux S, Alexander EK. Nontoxic diffuse goiter, nodular thyroid disorders, and thyroid malignancies. In: Melmed S, Auchus RJ, Goldfine AB, Koenig RJ, Rosen CJ, eds. Williams Textbook of Endocrinology. 14th ed. Philadelphia, PA: Elsevier; 2020:chap 14.
Paschke R, Eszlinger M, Kopp P. Euthyroid and hyperthyroid nodules and goiter. In: Robertson RP, ed. DeGroot's Endocrinology. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 77.
Pearce EN, Hollenberg AN. Thyroid. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 207.
Smith JR, Wassner AJ. Goiter. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 583.
Thyroid enlargement - scintiscan - illustration
Thyroid enlargement - scintiscan
illustration
Thyroid gland - illustration
Thyroid gland
illustration
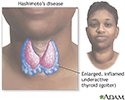
Hashimoto's disease (chronic thyroiditis) - illustration
Hashimoto's disease (chronic thyroiditis)
illustration
Review Date: 2/28/2024
Reviewed By: Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.